
Covid Pedia
Overcounting Deaths and Hospitalizations
Throughout the COVID era, experts and laymen discussed the latest numbers of COVID infections, hospitalizations, and deaths. News outlets reported these numbers constantly as policymakers instituted lockdowns, social distancing, and mask mandates based on the reported COVID data. But what exactly was a "COVID hospitalization" or a "COVID death" and were these numbers an accurate reflection of the effects of COVID?
The integrity of the data is critical to get an accurate picture. In many areas of the world, COVID may have been under-reported due to a lack of diagnosis, access to medical care, or reporting systems. However, in the Western world, over-reporting occurred in several ways.
Presumed COVID
Early on, deaths were reported as COVID even if no test was performed. According to the WHO guidelines, it was sufficient that there was a “clinically compatible illness" that was “a probable” COVID case, and doctors were instructed to "always apply these instructions, whether they can be considered medically correct or not." [1]
The CDC allowed COVID deaths to include “probable” or “presumed” diagnoses of COVID, even if there was no positive lab test.[2]
This broad and ambiguous definition led to deaths being labeled as COVID when COVID may not have even been present or when it had played a minor role in the patient's death. By mid-April 2020 nearly 37% of COVID deaths in New York City were found to be “presumptive” COVID deaths.[3]
Doctors have leeway in recording deaths. Montana Dr. Annie Bukacek explained that, even before COVID, doctors had leeway in recording the cause of death and that “more often than we like to admit, we don’t know with certainty the cause of deaths when we fill out death certificates . . . and even when an autopsy is done, the cause of death is not always clear”.[4] The WHO and CDC try to standardize reports , but ultimately it is a judgment call.
Senator Dr. Scott Jensen also stated publicly that he felt that the recording of causation on death certificates was being handled differently than prior to COVID, in a way that increased the apparent mortality from COVID.[5] Later retrospective analysis would indeed confirm that many deaths were not really COVID deaths (see below).
In an April 2020 interview, quickly removed by YouTube, California physician Dr. Dan Erickson reported that ER colleagues told him they were being pressured to add COVID to death certificates.[6]
That same month, Project Veritas interviewed funeral home directors who were convinced that many of those officially recorded as dead from COVID were not actually COVID deaths. Brooklyn’s Schaeffer Funeral Home Director Joseph Antioco , said, “They’re putting everything as COVID-19, so they’re padding the numbers.”[7]
Josephine Dimiceli of Dimiceli & Sons Funeral Home, called a nursing home asking if the deceased had really died of COVID and the response she received was, “[W]ell, no. It was a failure to thrive. But we’re assuming they all have it [COVID]"[8]
CDC itself understood they would be overcounting, stating in a report, “[T]he rules for coding and selection of the underlying cause of death are expected to result in COVID-19 being the underlying cause more often than not.”[9]
From an epidemiological or academic standpoint that might be justifiable for the purpose of studying the pandemic, but not for making dramatic public policy decisions.
“Inadvertently overstating risk can make the anxious more anxious and the skeptical more skeptical.”[10]
-Dr Robin Dretler
Why overcount?
The decision to include COVID on a death certificate can also be influenced by other factors. There is a phenomenon known as “availability bias” where people make decisions based on what they are most familiar with — the most available explanation — which certainly includes the virus everyone was talking about. A doctor is more inclined to diagnose COVID when everyone around him is talking about and preparing for it.[11] Once COVID becomes a common and even expected diagnosis, peer pressure can also become a factor.
Administrative pressure could also have played a role since there were financial incentives to ascribe deaths to COVID. In June 2020 New York Times journalist Alex Berenson received a letter from a senior executive of a large Texas emergency medical chain. The executive had "heard several stories of how discharge planners are being pressured to put COVID as primary diagnosis — as that pays significantly better."[12]
The U.S. CARES Act granted a 20% add-on payment for hospitals providing inpatient care to Medicare patients diagnosed with COVID-19.[13] Medicare is the federal healthcare program serving people 65 and over — the population of patients most susceptible to being incorrectly labeled as COVID.
These payments were meant to offset the cost of COVID patient care, but, as Senator Scott Jenson said, “[A]nytime healthcare intersects with dollars, it gets awkward."[14] Doctors and hospital administrators are human and therefore susceptible to the influence of monetary gain, especially when the hospital is running on a tight budget in an emergency. Even if a patient is not clearly diagnosable for COVID but required similar care, it is financially advantageous for the hospital to list COVID on the death certificate since it is permissible under the guidelines.
Doctors may also have compassionate motives to include COVID on a death certificate. In India there were “huge monetary benefits” for the families of “COVID warriors” who died from COVID, unintentionally providing an incentive for the inclusion of COVID on death certificates.[15]
In the U.S., too, Congress passed the Coronavirus Response and Relief Supplemental Appropriations Act at the end of 2020. This new law authorized the Federal Emergency Management Agency (FEMA) to reimburse citizens for funeral expenses incurred for deaths related to COVID-19 on or after January 20, 2020.[16]
Such benefits could likely influence doctors to record a death as COVID even if the diagnosis was uncertain or unconfirmed simply out of compassion for the surviving family.
Financial incentives for COVID deaths were an unprecedented act, as Jay Bhattacharya and Kyle Lamb write in a January 2023, Newsweek article:
We are sympathetic to the plight of families who have lost a loved one due to COVID. But why extend benefits for just COVID? Why not make the same consideration for victims of cancer, heart disease, stroke, or the flu? Is a COVID death worse than death from these other diseases? If Congress wants to create a new federal funeral benefit, it should do so equitably so that the government treats every death equally.[17]
Inflating child hospitalizations was also done “to motivate pediatricians and families to seek the protection of vaccination” as admitted by New York State’s acting health commissioner, Mary Bassett.
There were many motives for broadly applying "COVID" to deaths beyond the glaring desire of government officials fanning the flames of fear to get the public to obey their policy pronouncements. Epidemiologists wanted to get as much information as possible. Hospital administrators wanted to take advantage of available monetary assistance from government agencies. Doctors wanted to help the families of their patients, who might miss out on financial aid without the diagnosis. The end result is the same: more deaths were recorded as COVID deaths than can be proven.
Comorbidities
The second way in which COVID was overcounted is more complicated and nuanced. Since COVID is most severe in the elderly and those with serious chronic health conditions, it is genuinely difficult to determine to what degree COVID was responsible for a given death or hospitalization. There were many cases where patients were very elderly with multiple illnesses, and not expected to live much longer contracted COVID and died.
“COVID is a syndemic, where most deaths occur in people with several underlying diseases. Dissecting the relative contribution of each disease/condition to death can be difficult.”[18]
The CDC reported that only about 6% of COVID deaths had no comorbidities.[19] Meaning that 94% of COVID deaths had additional contributing causes of death listed on the death certificate.[20]
According to a UK study over the summer of 2020, nearly a third of all deaths recorded as COVID did not have COVID as an “underlying cause of death”.[21] That figure appears to be consistent with other time periods as well.[22]
Similarly in Italy, the scientific adviser to Italy’s minister of health said that “Only 12 percent of death certificates have shown a direct causality from coronavirus.”[23] This is not a surprise since the average age of a COVID death was above life expectancy.[24]
With COVID, not from COVID
The third way COVID was overcounted was as a result of mass PCR testing. Testing was so widespread that in the 2020–2021 season the US conducted over 585 million tests for COVID.[25] By contrast, a typical season sees an average of 77,000 tests for flu.[26] People were getting tested using the free and widely available PCR tests for many non-clinical reasons including having been in close contact with another PCR-positive person, in order to leave quarantine or to board an airplane.
Many hospitals routinely tested new patients even if they didn't present with COVID symptoms.[27] The massive testing meant that there were large sections of the population who tested positive yet were asymptomatic or had mild symptoms. If any of them were hospitalized they were considered COVID hospitalizations, and if they died, were considered COVID deaths. This is known as "with COVID" cases as opposed to those who were hospitalized or died "from COVID".
Public health officials and the media generally counted the "with COVID" and the "from COVID" as one group. In the UK, COVID deaths were counted as "occurring within 28 days of a positive test".[28] In Denmark, "all deaths for which a positive COVID-19 PCR test was recorded within the 30 days leading up to the date of death are counted as COVID-19 deaths."[29]
This unprecedented use of mass testing and broad definition of COVID cases, hospitalizations, and deaths was acknowledged by many public health officials.
White House Coronavirus Response Coordinator Dr. Deborah Birx said, "The intent is . . . if someone dies with COVID-19, we are counting that.”[30]
Ontario Ministry of Health Senior Communications Advisor Anna Miller said, “A death that occurs in an active case of COVID-19 is counted as a COVID-19 death.”[31]
Toronto Public Health Twitter account tweeted, “Individuals who have died with COVID-19, but not as a result of COVID-19 are included in the case counts for COVID-19 deaths in Toronto.”[32]
White House COVID-19 adviser Dr. Anthony Fauci said, “If you look at the children who are hospitalized, many of them are hospitalized with COVID as opposed to because of COVID.”[33]
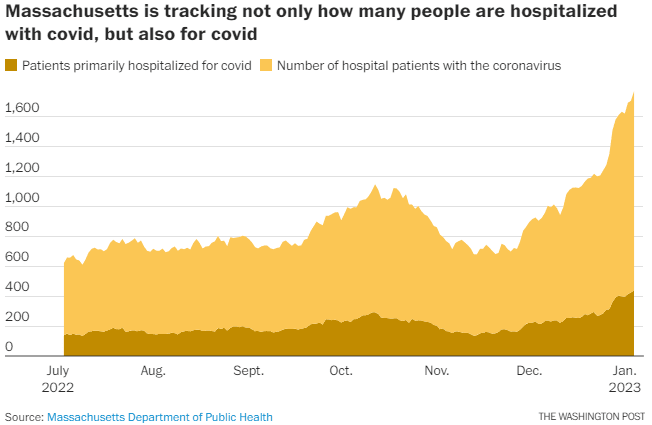
Massachusetts Public Health Commissioner Margret Cooke admitted that "our approach proved to be too expansive and led to a significant overcount of deaths in Massachusetts.”[34]
How significant?
The exact extent to which the COVID numbers were overcounted is impossible to know and studies on the topic are limited. One study looked at autopsy results of "COVID" deaths and found that "COVID-19 as the underlying cause of death in 86% of the autopsy cases, whereas in 14% COVID-19 was a concomitant disease."[35]
However, the cause of death listed on death certificates is often flawed even prior to COVID so the cause of death always needs to be taken with a grain of salt. One study investigating errors on death certificates showed 82% of death certificates contained one or more errors,[36] and a substantial discrepancy between the diagnoses on death certificates compared with autopsy. [37] For example, death certificates of 433 autopsied hospital patients in Iceland matched against post-mortem examinations showed significant discrepancies in 50% of patients and incorrectly stated the immediate cause of death in 25%.[38] [39]
The reason for hospitalizations is also murky, especially among the very elderly, or those with chronic illnesses. However, one study involving hospitalizations under Veterans Affairs in the US found "the proportion with moderate-to-severe [COVID] disease (as defined by the NIH [40]) before widespread vaccine availability was 64.0%." [41] Meaning the other 36% of "COVID patients" were likely in the hospital for other reasons.
Once the state of Massachusetts started listing hospitalizations "for" COVID and "with" COVID separately, it became clear that patients who were hospitalized "for" COVID represented less than a third of the total COVID patients.
In the UK, The Telegraph reported, based on leaked NHS data that "the majority of [COVID] cases [56%] were not detected until patients underwent standard COVID tests, carried out on everyone admitted to hospital for any reason."[42]
Similarly, in New York State, during the Omicron wave, hospital data revealed that "COVID was not included as one of the reasons for admission in 43 percent of current 'COVID hospitalizations'. These patients 'with' COVID, were hospitalized for unrelated reasons but tested positive for the virus on the routine screening administered to all new patients and were subsequently reclassified as COVID admissions. In New York City the figure was 51%.[43]
For children hospitalized as "COVID patients", the results are starker. One study looked at COVID patients in America's fifth-largest children’s hospital and found that out of 146 records listing patients as positive for SARS-CoV-2 from May 1, 2020, to September 30, 2020, the authors classified 58 (40 percent) as having “incidental” diagnosis. "Patients had incidental infection (40%), were potentially symptomatic (47%), or were significantly symptomatic (14%)."[44]
Another study looked at children hospitalized in Northern California and found that among the 117 pediatric SARS-CoV2-positive patients hospitalized between May 10, 2020, and February 10, 2021, 53 of them (or 45 percent) “were unlikely to be caused by SARS-CoV-2.” The authors concluded that "reported hospitalization rates likely lead to overestimation of the true disease burden."[45]
Revisions & admissions
After much of this data came to light, and after panicked-based policies were already enacted, public health officials began revising their COVID numbers downward.
Santa Clara County, California revised the official COVID death toll down by 22% [46] after it "refined its approach in reporting the data". Alameda County, California lowered its COVID death count by 25%. [47]
After an investigation by the Freedom Foundation, Washington State admitted 13% of COVID deaths were not really COVID deaths.[48]
The Province of Ontario admitted that "around 10% of COVID deaths are in fact “cause of death unknown or missing”. They also acknowledged that "[b]etween 10-20% of Ontario’s deaths (depending on the wave) are classified as ’deaths due to chronic or other pre-existing conditions that were exacerbated by COVID.’” [49]
In Massachusetts, after implementing a "new measuring criteria," it reduced the number of COVID deaths by about 15 percent.[50]
Colorado health officials changed how they "count the number of people lost to the coronavirus outbreak" and revised numbers downward by 24%.[51]
CDC discovered a “coding logic error” that was accidentally counting 'COVID' deaths that were not actually COVID, this error added more than 72,000 COVID deaths of all ages — or about 7% of the total number of deaths.[52]
In the UK, the Office for National Statistics (ONS) revealed that 23% of COVID-19 deaths were listed as 'with' the disease rather than 'from' the disease.[53]
Clearly, the highly flawed method of counting COVID deaths and hospitalizations leads directly to overcounting. While it's hard to know exactly how much the numbers have been inflated, estimates that have been acknowledged by public health authorities range from 7% up to 25% of deaths, and 14% to 56% of hospitalizations. The result is a significant overestimation of the true impact of the virus and contributed to panic-based policies.
Email questions or comments to [email protected]
Footnotes:
[1] https://web.archive.org/web/20200424163455/https:/www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf?ua=1 (page 3 & page 8 at the bottom)
[2] "These can include laboratory confirmed cases, as well as cases without laboratory confirmation."
https://www.cdc.gov/nchs/nvss/vsrr/covid19/tech_notes.htm
[3] “More than 3,700 additional people who were presumed to have died of the coronavirus”
https://www.nytimes.com/2020/04/14/nyregion/new-york-coronavirus-deaths.html
[4] https://www.youtube.com/watch?v=_5wn1qs_bBk&t=1041s&ab_channel=LibertyFellowshipMT , Minute 4:30
[5] https://www.valleynewslive.com/content/news/MN-Sen-Dr--569489461.html
[6] https://rumble.com/v1isy2j-covid-19-press-conference-interview-with-dr.-dan-erickson-and-dr.-artin-mas.html
Minute 30:45
[7] https://web.archive.org/web/20200501085436/https://www.projectveritas.com/news/breaking-funeral-directors-in-covid-19-epicenter-doubt-legitimacy-of-deaths/
[8] https://pjmedia.com/blog/megan-fox/2020/04/30/nyc-funeral-directors-reveal-shocking-inflation-of-covid-19-deaths-n387013
[9]https://www.cdc.gov/nchs/data/bsc/bsc-pres-Sutton-May-5-2020.pptx (Slide 8)
https://www.youtube.com/watch?v=_5wn1qs_bBk&t=1041s minute 12:05
[10] https://www.washingtonpost.com/opinions/2023/01/13/covid-pandemic-deaths-hospitalizations-overcounting/
[11] "Availability heuristic or availability bias can inadvertently affect patient outcomes. These biases may be magnified during times of heightened awareness of a particular disease."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9273171/
[12] https://twitter.com/AlexBerenson/status/1277773122301804546
[13] https://www.aha.org/advisory/2020-04-16-coronavirus-update-cms-releases-guidance-implementing-cares-act-provisions
[14] https://rumble.com/vl0cn5-dr.-scott-jensen-with-laura-ingraham-the-ridiculous-cdc-guidlines.html
minute 3:10
[15] ”Also some of the state governments announced the huge monetary compensations to the tune of INR 10 million (1,40,000$) for the so called 'Corona Warriors’ that is health care workers, police personnel etc., who die due to COVID-19, while on duty."
[16] https://www.fema.gov/disaster/historic/coronavirus/economic/funeral-assistance/faq
[17] https://www.newsweek.com/downsides-financial-incentives-diagnose-covid-opinion-1776181
[18] https://link.springer.com/article/10.1007/s10654-021-00787-9 (under Challenges in syndemic death counting)
[19] “CDC report shows 94% of COVID-19 deaths in U.S. had contributing conditions”
[20] https://abc-7.com/news/2020/08/31/cdc-report-shows-94-of-covid-19-deaths-in-u-s-had-contributing-conditions/
[21] “This proportion has risen substantially to nearly a third over the last eight weeks”
https://www.cebm.net/covid-19/death-certificate-data-covid-19-as-the-underlying-cause-of-death/
[22] https://www.dailymail.co.uk/news/article-9467793/Covid-lockdown-UK-Nearly-quarter-people-dying-Covid-NOT-killed-virus.html
[23] https://www.uniba-partners.com/fileadmin/uploads/uniba/Documents/COVID-19/2020_03_30_The_mystery_of_the_true_coronavirus_death_rate___Financial_Times.pdf
[24] 64.58% of COVID-related deaths were above life expectancy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8057856/
[25] https://ourworldindata.org/grapher/full-list-total-tests-for-covid-19?time=2020-10-01..2021-09-30&country=~USA
[26] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6038762/#:~:text=Number%20of%20influenza%20tests%20reported,specimens%20has%20been%20tested%20annually.
[27] https://www.hsj.co.uk/coronavirus/all-hospital-emergency-patients-to-be-tested-for-coronavirus/7027526.article
https://www.uwmedicine.org/coronavirus/safety/inpatient-screening
[28]https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronavirusCOVID19latestinsights/deaths
[29] https://en.ssi.dk/news/news/2022/mortality-due-to-covid-19-in-denmark-is-not-increasing-as-much-as-are-case-numbers
[30] https://nypost.com/2020/04/07/feds-classify-all-coronavirus-patient-deaths-as-covid-19-deaths/
https://www.rev.com/blog/transcripts/donald-trump-coronavirus-task-force-briefing-april-7
[31] https://tnc.news/2020/12/13/ontario-counts-suicide-victims-as-covid-19-fatalities/
[32] https://twitter.com/TOPublicHealth/status/1275888390060285967?_gl=1*1lcu9ac*_ga*MTk1NTU2NzkxNS4xNjg2MTU3Nzcy*_ga_RLBBDN7YJL*MTY4NzIwMjIzNi4zLjAuMTY4NzIwMjIzNi42MC4wLjA.
[33] https://www.theepochtimes.com/fauci-hospitals-are-overcounting-covid-19-cases-in-children_4187345.html
[34] https://www.theepochtimes.com/massachusetts-to-reduce-significant-overcount-of-covid-19-deaths_4330491.html
[35] https://www.sciencedirect.com/science/article/pii/S2666776222000230?via%3Dihub
[36] https://pubmed.ncbi.nlm.nih.gov/16253030/
[37] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1769693/
[38] https://pubmed.ncbi.nlm.nih.gov/1871957/
[39] https://www.medrxiv.org/content/10.1101/2022.04.28.22274344v1.full
[40] https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/
[41] https://www.researchsquare.com/article/rs-898254/v2?redirect=/article/rs-898254
[42] https://www.telegraph.co.uk/news/2021/07/26/exclusive-half-covid-hospitalisations-tested-positive-admission/
[43] https://www.dailymail.co.uk/news/article-10381687/New-York-hospitals-admit-nearly-HALF-COVID-patients-admitted-unrelated-maladies.html
[44] https://publications.aap.org/hospitalpediatrics/article/11/8/e133/179737/Characteristics-of-Hospitalized-Children-Positive
[45] https://publications.aap.org/hospitalpediatrics/article/11/8/e151/179740/For-COVID-or-With-COVID-Classification-of-SARS-CoV
[46] https://www.cbsnews.com/sanfrancisco/news/santa-clara-county-revises-covid-death-toll-down/
[47] https://covid-19.acgov.org/covid19-assets/docs/press/press-release-2021.06.04.pdf
[48] https://www.freedomfoundation.com/washington/wa-officials-freedom-foundation-correct-about-over-counted-covid-19-deaths-but-still-havent-corrected-method/
[49] https://torontosun.com/opinion/columnists/furey-ontario-reveals-deaths-caused-by-covid-much-lower-than-previously-reported
[50] https://www.theepochtimes.com/massachusetts-to-reduce-significant-overcount-of-covid-19-deaths_4330491.html
[51] https://www.coloradoan.com/story/news/2020/05/16/colorado-changes-how-coronavirus-deaths-state-counted/5198485002/
[52] https://www.theguardian.com/world/2022/mar/24/cdc-coding-error-overcount-covid-deaths
[53] https://www.dailymail.co.uk/news/article-9467793/Covid-lockdown-UK-Nearly-quarter-people-dying-Covid-NOT-killed-virus.html
https://www.telegraph.co.uk/news/2021/04/13/quarter-covid-deaths-not-caused-virus/